Descripción de pacientes con síndrome de Guillain Barré. Hospital pediátrico José Luis Miranda. 2008-2012
Palabras clave:
parálisis; paralysis; parálisis respiratoria; respiratory paralysis; paresia; paresisResumen
RESUMEN
Introducción: El Síndrome de Guillain–Barré es una causa frecuente de parálisis motora aguda generalizada en niños de países donde la poliomielitis ha sido erradicada, como Cuba y el mundo occidental.
Objetivo: Caracterizar los pacientes con Síndrome de Guillain Barré en el hospital José Luis Miranda en el período 2008-2012.
Diseño Metodológico: Se realizó un estudio observacional descriptivo de corte transversal. El universo estuvo constituido por 12 pacientes.
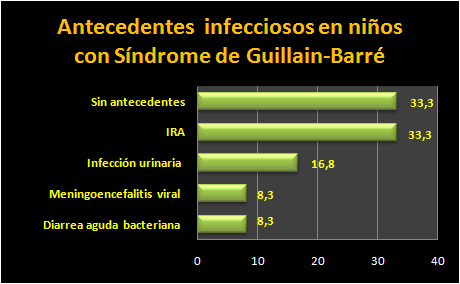
Resultados: El grupo de edad más representado fue el de 4 a 7 años con un 50 %. El sexo masculino predominó en un 83,3 %. Los principales antecedentes infecciosos correspondieron con infección respiratoria alta (33,3 %) e infección del tracto urinario (8,3 %). 5 pacientes presentaron complicaciones y uno de estos falleció.
Conclusiones: La mayor parte de los pacientes del estudio pertenecieron al grupo de edad de 4 a 7 años, del sexo masculino. Los antecedentes infecciosos más llamativos fueron las Infecciones respiratorias altas. La mayoría de los pacientes tuvo evolución favorable.
ABSTRACT
Introduction: The Guillain-Barre Syndrome is a frequent cause of generalized acute motor paralysis in children of countries where the poliomyelitis has been eradicated, as Cuba and the western world.
Objective: To characterize the patients with Guillain-Barre Syndrome in the hospital José Luis Miranda in the period 2008-2012.
Material and methods: An observational, descriptive and traverse study was carried out. The universe was constituted by 12 patients.
Results: The represented age group went the one from 4 to 7 years with 50 %. The masculine sex prevailed in 83, 3 %. The main infectious antecedents corresponded with high breathing infection (33, 3 %) and infection of the tract urinal (8,3 %). Five patients presented complications and one of these it died.
Conclusions: Most of the patients of the study belonged to the age group from 4 to 7 years, of the masculine sex. The most important infectious antecedents were the high breathing infections. Most of the patients had favorable evolution.
Key words: paralysis, respiratory paralysis, paresis.
Citas
Lestayo–O´Farrill Z, Hernández–Cáceres JL. Análisis del comportamiento del síndrome de Guillain–Barré. Consensos y discrepancias. Rev Neurol. 2008; 46: 230–7.
Cruse RP. Overview of Guillain-Barré syndrome in children. 2007; [citado 23 sept 2013]. Disponible en: URL:http://www.uptodate.com/
Bradshaw DY, Jones HR. Pseudo meningoencephalitic presentation of pediatric Guillain-Barré syndrome. J Children Neurol. 2001; 16:505-8.
Madrid Rodríguez A. Síndrome de Miller-Fisher asociado a neuropatía axonal motora aguda: correlación clínico-inmunológica. Neurología. 2012; 27(3):179-88.
Winer JB. Guillain-Barré syndrome. Revisión clínica. BMJ. 2008; 337:671.
Estrada–González JR, Goyenechea A, Herrera C. Brote de polirradiculoneuritis aguda tipo Landry–Guillain–Barré–Ströhl durante una epidemia de dengue. Rev Cub Hig Epidem. 1981; 19:252–65.
Asbury AK, Arnason BG, Karp KR, McFarlain DE. Criteria for diagnosis of Guillain Barré syndrome. Ann Neurol. 1978; 28(3):565-6.
Asbury AK. New concept of Guillain-Barré syndrome. J Child Neurol. 2000; 15:183-91.
Geleijns K, Brouwer BA, Jacobs BC, Houwing-Duistermaat JJ, van Duijn CM, van Doorn PA. The occurrence of Guillain-Barré syndrome within families. Neurology. 2004; 63:1747-50.
Ramírez–Zamora M, Burgos–Ganuza CR, Alas–Valle DA, Vergara–Galán PE, Ortez–González CI. Síndrome de Guillain–Barré en edad pediátrica. Perfil epidemiológico, clínico y terapéutico en un hospital de El Salvador. Rev Neurol. 2009; 48:292–6.
Kaida K, Kamakura K, Ogawa G, Ueda M, Motoyoshi K, Arita M, et al. S. GD1b- specific antibody induces ataxia in Guillain-Barré syndrome. Neurology. 2008; 71:196-201.
Rocha MS, Brucki SM, Carvalho AA, Lima UW. Epidemiologic features of Guillain-Barré syndrome in Sao Paulo, Brazil. Arq Neuropsiquiatric. 2004; 62:33-7.
Winner JB. Guillain–Barré syndrome: Clinical variants and their pathogenesis. Journal of Neuroimmunology. 2011; 231:70–72.
Kuwabara S. Guillain-Barré syndrome. Curr Neurol Neurosci Rep. 2007; 7:57-62.
McCoya B, Kinga M, Gillb D, Twomeyc E. Childhood posterior reversible encephalopathy syndrome. European Journal of Pediatric Neurology. 2011; 15(2):91-94.
Arami MA, Yazdchi M, Khandaghi R. Epidemiology and characteristics of Guillain-Barré syndrome in the northwest of Iran. Ann Saudi Med. 2006; 26:22-7.
McLean M, Duclos P, Jacob P, Humphreys P. Incidence of Guillain-Barré syndrome in Ontario and Quebec, 1983-1989,using hospital service data bases. Epidemiology. 1994; 5:443-8.
Ferreira R, Boto A, Correia M, Moreno T, Carvalho A, Santos E, et al. Síndrome de Guillain-Barré e hipertermia maligna: uma nova associação? Acta Pediatrica Portuguesa. 2002; 6:449-52.
López Jiménez E, Silveira Sánchez D, Ricardo Ojea L. Síndrome de Guillain-Barré en la Unidad de Cuidados Intensivos. Rev 16 de abril. 2010; 241
Monteiro JP, Fonseca J, Proenca P, Calhau M, Braga MJ. Síndrome de Guillain- Barré en edad pediátrica. Experiencia de la Unidad de Neuropediatría de un hospital portugués. Rev Neurol. 2006; 42(3):144-149.
Torriente Cortina M, Barroso AF, Valdivieso Romero JF. Caracterización del síndrome de Guillain–Barré en el Hospital “Julio Trigo López” durante el período 2000–2009. Rev Cubana Neurol y Neurocir. 2012; 2(1):3–8.
Pérez Lledó E, Díaz Vico A, Gómez Gosálvez FA. Síndrome de Guillain-Barré: presentación clínica y evolución en menores de 6 años de edad. An Pediatr (Barc). 2012; 76(2):69-76.
Vázquez Vázquez L, Gómez Vargas JR, Candales Arafet LA, Vázquez Drake A. Síndrome de Guillain-Barré-Strohl. Variedad Miller-Fisher. Rev Cubana Med Intens Emerg. 2005; 4(1).
Ostia Garza PJ, Fuentes Cuevas MC. Síndrome de Guillain-Barré variedad Miller-Fisher. Reporte de un caso. Arch Inv Mat Inf. 2011; 3(1):30-35.
Hughes RA, Raphael JC, Swan AV, van Doorn PA. Intravenous immunoglobulin for Guillain-Barré syndrome. Cochrane Data base Syst Rev. 2009 ;( 2).
Kuijf ML, Geleijns K, Ennaji N, van Rijs W, van Doorn PA, Jacobs BC. Susceptibility to Guillain–Barré syndrome is not associated with CD1A and CD1E gene polymorphisms J. Neuroimmunol. 2008; 35(7):49-57.
Fernández–Ortega JF, de Rojas–Román JP, Núñez–Castain MJ, Miralles–Martín E, Bravo–Utrera M. Síndrome de Guillain–Barré en Unidad de Cuidados Intensivos. Rev Neurol. 2001; 33:318–24.
Visser LH, Schmitz PI, Meulstee J, van Doorn PA, van der Meche FG. Prognostic factors of Guillain-Barré syndrome after intravenous immunoglobulin or plasma exchange. Dutch Guillain-Barré Study Group. Neurology. 2011; 53:598-604.
Sang D, Chen Q, Liu X, Hongdang Q, Daoxiang W, Liang Y, Zhang L. Fc receptor like 3 in Chinese patients of Han nationality with Guillain–Barré syndrome. Journal of Neuroimmunology. 2012; 246(1-2):65–68.
Kokubun N. Conduction block and axonal degeneration co-occurring in a patient with axonal Guillain-Barré syndrome. Journal of the Neurological Sciences. 2012; 319(1-2):164-167.
Descargas
Publicado
Cómo citar
Número
Sección
Licencia
Aquellos autores/as que tengan publicaciones con esta revista, aceptan los términos siguientes:
Los autores/as conservarán sus derechos de autor y garantizarán a la revista el derecho de primera publicación de su obra, el cuál estará bajo una Licencia de Creative Commons Reconocimiento-NoComercial 4.0 Internacional (CC BY-NC 4.0)
Los autores/as podrán adoptar otros acuerdos de licencia no exclusiva de distribución de la versión de la obra publicada (p. ej.: depositarla en un archivo telemático institucional o servidores preprint) siempre que se indique la publicación inicial en esta revista.
Se permite y recomienda a los autores/as difundir su obra a través de Internet (p. ej.: en archivos telemáticos institucionales o en su página web) antes y durante el proceso de envío, lo cual puede producir intercambios interesantes y aumentar las citas de la obra publicada.